
It is true that the basic function of your heart is to pump blood and supply oxygenated blood to your body tissues, but in reality, your heart is a complex body organ and so many factors determine how much blood is pumped through the body. Preload and afterload are two determinants of how much blood your heart pumps in a minute (cardiac output).
What Is Cardiac Output?
Before learning more about preload and afterload, it is important to learn a bit about cardiac output, which is measured in mL blood/min. The volume of blood pumped by your heart per minute is its cardiac output. It refers to the function of stroke volume and heart rate. The heart rate refers to the number of times your heart beats in a minute. The stroke volume refers to how much bloods get pumped out of heart with each beat. Cardiac output will increase if stroke volume or heart rate increases.
Cardiac output (mL per min) = heart rate (beats per min) x stroke volume (mL per beat)
A resting heart rate for an average person is 70bpm, whereas a resting stroke volume is 70 mL per beat. Using the above formula, an average person will have a cardiac output of 4900 mL per minute. Now, if you consider the total volume of blood in the circulatory system, which is around 5000mL, it will become clear that the heart of an average person pumps the entire volume of blood in the circulatory system after every minute.
Preload and After Load – Two Determinants of Cardiac Output
 The main goal of your heart is to circulate adequate amount of blood to your tissues to ensure they receive enough oxygen for proper functioning. However, your metabolic rate may have an impact on how much blood your heart needs to pump – with a change in your metabolic rate, there will be a change in the amount of oxygen required by your tissues. Basically, there are two determinants of cardiac output – preload and afterload. Here's more about these determinants.
The main goal of your heart is to circulate adequate amount of blood to your tissues to ensure they receive enough oxygen for proper functioning. However, your metabolic rate may have an impact on how much blood your heart needs to pump – with a change in your metabolic rate, there will be a change in the amount of oxygen required by your tissues. Basically, there are two determinants of cardiac output – preload and afterload. Here's more about these determinants.
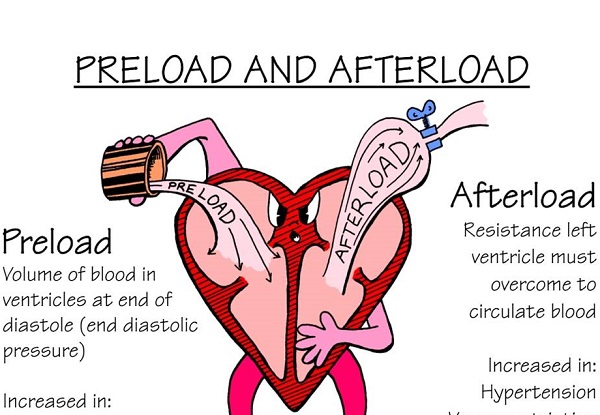
Preload
Preload is basically the stretch on the sarcomeres just before your heart contracts (systoles). The sarcomeres will stretch more if there is more blood in the chamber just before contraction. When sarcomeres are stretched further, the contraction will be equally strong. This will increase the stroke volume. If you ask the relationship between the strength of contraction and end-diastolic sarcomere length, there are two basic explanations. Initially, there is a greater chance for actin-myosin cross bridging; another explanation is that this happens because length dependent channels become activated in the process.
Afterload
Afterload refers to the stress or tension generated by the left ventricle wall during ejection of blood. Besides, the state of your blood vessels plays a big role in this process. Your blood vessels have the ability to dilate and constrict, which in turn help change the total resistance to blood flow. Afterload will get affected by this resistance. An important thing to understand is that your heart doesn't usually eject all blood it has, but ejects only 2/3 of the total blood available in its chamber at end-diastole. With an increase in afterload, not enough blood in the ventricle would move out. When afterload decreases, it allows more blood to leave the chamber. It implies that with an increase in afterload, stroke volume will decrease and vice versa.
Other Two Determinants of Cardiac Output
Preload and afterload are two of the major determinants of cardiac output, but there are 2 other factors may also affect the overall cardiac output.
Heart Rate
If your heart rate at rest is 50bpm, it means your heart would eject 100ml of blood with each beat. Remember, with other factors being equal (such as stroke volume maintains at 100 ml), if heart rate is raised, then cardiac output will be increased as well.
Contractility
It measures the performance of cardiac pump, the degree to which your muscle fibers may shorten when they are activated by certain stimulus independent of preload and afterload.If everything else remains constant and contractility increases, it will make the ventricle to eject more blood, which in turn will increase stroke volume. It implies that if preload and afterload stay unchanged, raising contractility will directly increase stroke volume and vice versa.
What About the Highs and Lows of Preload and Afterload
Cardiac output will get affected with the highs and lows of preload and afterload. Hypotension, shock and tamponade are some states when preload will be low. Sometimes, preload is low due to volume issue. This can be resolved by adding volume through blood and fluids. However, some states like brady-arrhythmias and heart failure will create excessive volume and lead to an increase in preload.
Similarly, afterload, which basically refers to vascular resistant within the lungs and aorta, may have highs and lows as well. Afterload is usually high during SNS stimulation, aortic stenosis and HTN. If that’s the case, you may benefit from vasodilators. Afterload will be low due to hypotension or sepsis. If that's the case, vasopressors may benefit the patient.