
A tracheostomy procedure involves inserting a tube either temporarily or permanently into a patient's windpipe so that they can breathe easier. A cut is made just below the vocal chords and the tube is inserted from the cut straight into the lungs. Air that is drawn into the body then bypasses the nose, mouth and throat, which can make it easier for people do breathe if there are blockages in these areas. A tracheostomy is often called a "stoma" which is also the name for the hole made in the throat where the tube is inserted.
Tracheostomy Procedure
Most often, the tracheostomy procedure is performed either in an operating room or in an intensive care unit. When having undergone the procedure, the patient is then continuously monitored for their oxygen saturation with a pulse oximeter and for their cardiac rhythm with an EKG (electrocardiogram).
Step 1
The vast majority of tracheostomy procedures are done when the patient is under local anaesthetic, although sometimes the patient can be safely intubated or ventilated with a mask. Generally, the procedure needs at least an anaesthetist and a surgeon. If the anaesthetist is unable to maintain a clear airway, the surgeon should be present at that time. Before the tube is introduced into the throat, the soft tissue, skin and the trachea (into the two lumen) should be injected or otherwise infiltrated with adrenaline and local anaesthesia. Whenever a tracheostomy procedure is performed, a complete set of tracheostomy instruments should be close at hand as the patient is anaesthetized, so, if necessary, the surgeon can convert to an emergency tracheostomy.
Step 2
The patient's neck must be carefully positioned so that access to the trachea is easy to find in order to make the procedure as safe as possible. To achieve this, the neck is usually extended over a shoulder roll, exposing the throat. The anaesthetist usually stands close to the patient's head and places the endotracheal tube (or the ETT) using a direct laryngoscopy, ensuring that the cuff is halfway at the same level as the vocal chords.
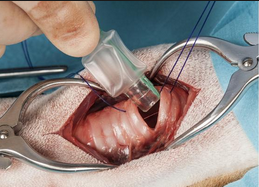
Step 3
Once everything is ready and the patient has been adequately prepared, the anaesthetist usually injects the area where the tracheostomy procedure will be performed with anaesthesia. Once the patient can no longer feel anything, a horizontal or even vertical incision is made which usually measures around three to four centimeters in length.
Step 4
Before the tube is inserted into the incision that has been made, the surgeon performs a minimal dissection. During this part of the procedure, the thyroid isthmus is pushed downward and the larynx is stabilized. The surgeon will then perform a bronchoscopy and the best site for the introducer needle is found. The tip of this needle is pushed into the tracheal lumen, ensuring that it does not touch or pierce the posterior tracheal wall.
Step 5
As the cannula is kept in the tracheal lumen, the needle is withdrawn and then a J-tipped wire is positioned. A stylet is then also positioned, ensuring that its safety ridge is directed towards the tip of the wire. In order to make access easier for the surgeons to perform the procedure, the tract is dilated. The dilator that is used - often a Blue Rhino dilator, is loaded onto the stylet which has been previously positioned, with its tip resting on the safety ridge. This dilator can then easily be moved in and out in order to dilate the tissues between the tracheal lumen and skin to the optimal size when adjust is as needed. However, the dilator is never pushed beyond the point when the 40 FR mark disappears.
Step 6
At this point, the surgeon will load a tracheostomy tube onto the dilator. Different sizes are usually used depending on the person, but gradually for women, a size six tracheostomy tube is used and for men a size eight is used. The dilator is then moved onto the safety ridge of the stylet and is positioned into the tracheal lumen. The surgeon should be able to see it at all times during this part of the procedure.
Step 7
Once the tracheostomy tube is in place, the bronchoscope can be withdrawn from the ETT. The tracheostomy tube can then be used to introduce the bronchoscope into the correct position, which is checked by the surgeon.
Step 8
Finally, the tube is secured with 2 sutures of 2-0 nylon. In most cases, tracheostomy tape is also used so that the tube does not slip or dislodge with movement. Additionally, the tracheostomy tube is connected to a flexible extension tube which links it to the ventilator circuit and which can reduce excess movement of the tube when the patient is postoperative care, for instance.
Below is a video you can know the procedure directly.
Follow-Up Care After Tracheostomy Procedure
Once a tracheostomy has been performed, antibiotics are typically prescribed to the patient in order to reduce the risk of the incision site getting infected. For those patients who are unable to breathe by themselves, the tracheostomy tube can also be linked up to a ventilator, which supplies a patient with oxygen and helps them to breathe so that enough oxygen can get to the lungs.
Immediately after the tracheostomy procedure, doctors will monitor the patient for several days. The tube that is placed into the trachea during the surgery will be changed around 10 to 14 days following the procedure. Any further changes will usually be the noted bythe nursing staff or the physician in charge of patient care.
For those with a temporary tracheostomy, the incision in the neck will be covered when the tube is removed. The incision will usually heal after a couple of weeks, leaving behind a small scar. Patients with a permanent tracheostomy need to be helped to get used to cleaning and maintaining their stoma, and helps and advices will also be given by the patient's doctor.