
Vertigo is a common problem, especially among older adults. It is defined as a feeling of dizziness accompanied by a sensation of spinning or tilting that cannot be controlled. If it is not caused by any specific disease, it is medically called benign paroxysmal positional vertigo (BPPV), and it is usually associated with a problem in one’s inner ear. Vertigo usually occurs when you suddenly turn your head or when you change position such as when you roll over in bed or tilt your head back.
An easy test to determine if your condition is due to BPPV is to do a Dix Hallpike maneuver, which involves testing if vertigo occurs when you turn your head a certain way. Your doctor will also observe if your eyes produce involuntary movements (nystagmus) during the test. This helps determine if the cause of your vertigo is due to a problem in the brain (central vertigo) or due to a problem in the inner ear (peripheral vertigo).
How Is Dix Hallpike Maneuver Done?
The maneuver helps identify the cause of vertigo – whether it is in your inner ear or your brain. If in the ear, it also determines which side is affected.This test can be uncomfortable because it reproduces your vertigo and may cause nausea. However, it is easy and inexpensive, so it may be done as part of your physical exam during a doctor’s visit.
What to Expect
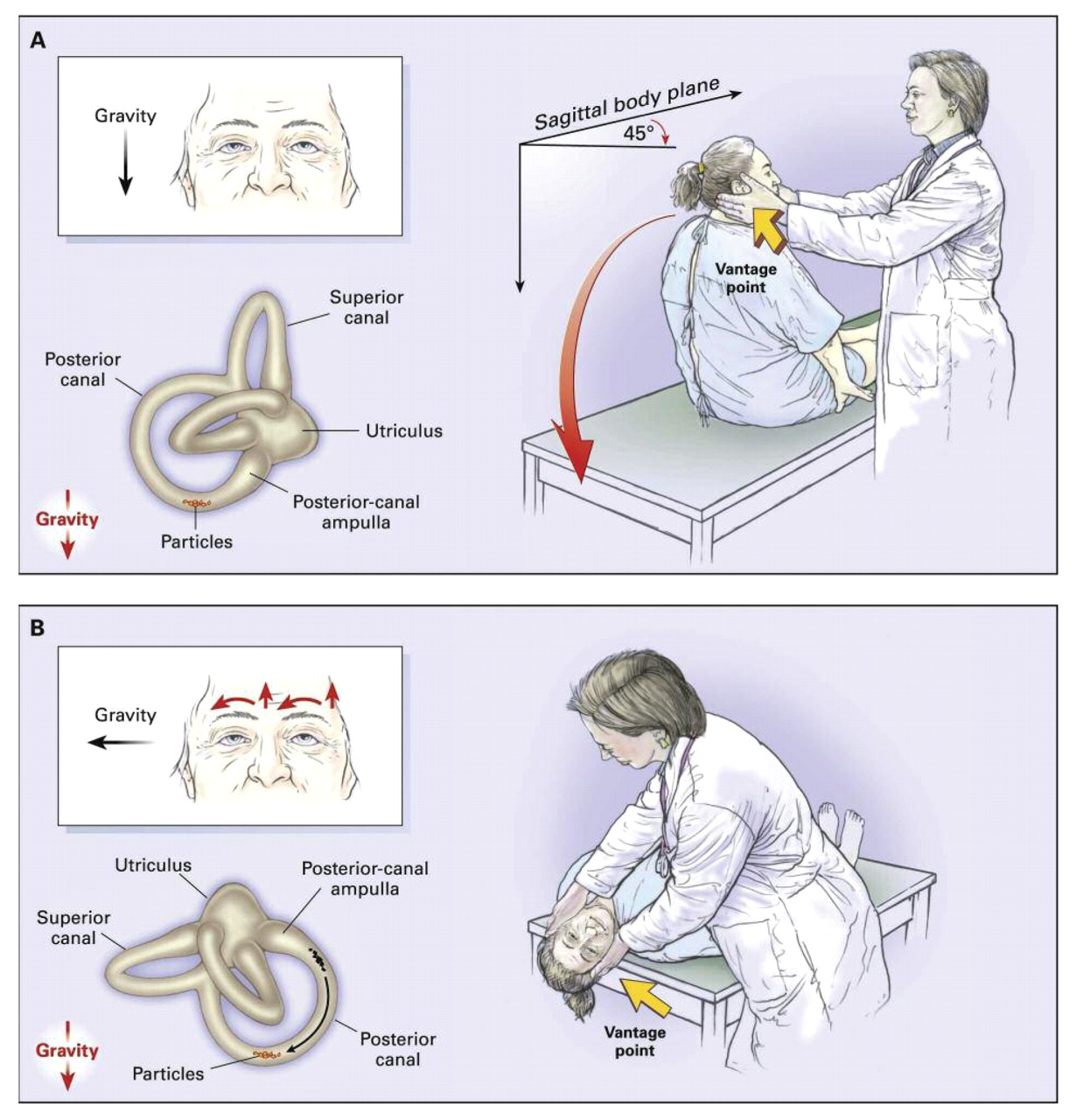
- During the maneuver, you will be asked to sit with your legs straight on an examination table. Your doctor will turn your head 30º - 45º to one side, then help you quickly lie back with your head hanging over at the end of the table.
- Your doctor will watch your eyes and observe for involuntary movements (nystagmus), which will help identify the cause of your vertigo.
- Then you will be asked to sit upright to recover from vertigo, and the procedure is repeated in the opposite direction.
Detailed Instructions for Healthcare Providers
1. The Dix Hallpike maneuver should only be done by those who have had proper training.
2. It begins by explaining the procedure to your patient and demonstrating it if necessary. Explain carefully that some dizziness may be experienced but this is likely to be temporary. Obtain patient’s consent before proceeding with the test.
3. Sit the patient on the examination table in a position such that when he lies down, his shoulders will fall at a level at the end of the table.
4. If the patient’s history suggests BPPV, then start with the ear that is least involved. If there is no laterality, then either ear may be tested first.
5. Hold both sides of patient's head with your hands and turn it 45° towards one side.
6. Instruct the patient to fix his eyes on a point directly in front of him throughout the maneuver. Observe his eyes and note any nystagmus or other eye movements.
7. Instruct patient that on a count of 3, you will bring his torso and head backward quickly so that his head will go over the end of the table with your support all the time. He must keep his eyes open all the time and try to suppress blinks.
8. Repeat Dix Hallpike maneuver on the other side. When vertigo is induced, the patient may feel quite unsteady for a few minutes. Maintain physical contact with your patient when moving to the other side of the table. Place a reassuring hand on his shoulder. On completing the test, instruct patient to be careful when standing up.
Videos that show how the maneuver is done:
Precautions
- The Dix–Hallpike maneuver may cause stress on the patient’s lower back, so practice caution when dealing with patients who are suffering from low back pain.
- Patients with significant cardiac or respiratory problems may not be able to tolerate the maneuver.
Limitations
- A negative result does not predict the absence of BPPV a hundred percent. Some patients with BPPV will have negative test results. The Dix–Hallpike maneuver is only 79% sensitive and 75% specific.
- You can do the test more than once since it is not easy to demonstrate nystagmus typical of BPPV. The results may also be affected by the speed it is done in and the plane where the head is placed.
Dix Hallpike Maneuver Results
A normal result means that your vertigo or nystagmus did not occur during the test. Abnormal test results occur if you had vertigo or nystagmus during your test, which may be due to an inner ear problem or a brain problem.
Positive test
Characteristics of a positive test include:
- A 5–10 second latency of onset occurs.
- Rotational nystagmus or upbeating/downbeating nystagmus occurs. Central nervous system dysfunction is suggested by the presence ofupbeating/downbeating nystagmus without rotational nystagmus.
- Upbeating/downbeating nystagmus indicates whether vertigo is caused by a problem in the posterior semicircular canal of the tested, lower ear (upbeating) or the anterior semicircular canal of the upper ear, the contralateral side (downbeating).
- Multiple repetitions of this test will result in less nystagmus.
- After a positive maneuver, the direction of nystagmus will reverse upon sitting for a brief period.
To complete the Dix–Hallpike maneuver, bring the patient back to sitting position, and examine the eyes again. See if reversal occurs. Nystagmus may be paroxysmal and may be delayed for several seconds after performing the maneuver.
Negative Test
A negative test result indicates that BPPV is less likely and central nervous system problem must be considered.